By A Midwestern Doctor
The Forgotten Side of Medicine
September 29, 2025
During the COVID-19 rollout, patients gradually began to realize that some of the COVID-19 vaccines were more dangerous than others. Initially this was written off as a conspiracy theory. However, as time moved forward, and more evidence emerged to support the "hot lot" hypothesis there was an increasing acceptance of this theory.
At the time, the most common theory I heard raised to account for this was that a large global experiment was being done to assess the effects of various mRNA doses (e.g., one researcher was able to show that the hot lots of each COVID vaccine brand hit the market at different times in a manner that seemed to be coordinated between the manufacturers and that Pfizer's lots contained a simple code that correlated to their toxicity).
However, while this was possible (as you can put nothing past these people) I was more inclined to an alternative hypothesis: that it was not possible to correctly produce the mRNA vaccines at scale, so there would be a large number of production issues including many either toxic or inactive lots hitting the market.
This theory was based on both my knowledge of the specific engineering challenges the mRNA technology faced and the fact that hot lots are an enduring problem with vaccines.
Because of this, many (myself included) believe the vaccine industry concluded it wasn't possible to completely clean up their production process while maintaining the economic viability of the vaccines, so they instead focused on getting the Federal government to exempt them from liability for their hot lots under the argument that "vaccines were essential for our national security" so a certain number of people being injured by defective vaccines was an acceptable trade-off to maintain this "vital" national resource.
Given the severity of this allegation, I will now present several incidents where 'hot' vaccine lots have been identified in the market.
Adventitious Agents
One of the greatest challenges with producing a biological pharmaceutical is that it has to be grown in a medium (e.g., a virus within cells or a growth medium for bacteria). This introduces a few major issues.
• First, if cell cultures are used, an unrecognized virus may already have infected the cells and contaminated the final product.
• Second, anytime a growth medium is used, unwanted pathogens can also get in (e.g., from the air) and then grow there. This is especially problematic because the same labs that produce these products also often house harmful infectious organisms.
• The entire process inevitably requires a purification stage where the undesired contaminants (e.g., unwanted bacteria, foreign DNA, or toxic components of now destroyed bacteria) are removed. Unfortunately, it is often quite difficult or costly to remove these unwanted contaminants, and the cost frequently exceeds what the manufacturers are willing to pay.
In turn, unwanted biological contaminants (euphemistically termed adventitious agents) are an enduring challenge for the pharmaceutical industry. For example, this recent 2022 review paper highlighted some of the most common "adventitious agents" (e.g., mycoplasma frequently contaminate cultures) and cited a few well-known incidents such as:
• In 1946, a sheep vaccine was contaminated with prions (due to it being sourced from sheep in the early asymptomatic stage of the prion disease scrapie-something similar to Mad Cow Disease), which in turn caused the sheep in the herd that received the vaccine to later get scrapie.
• The FDA reported in 1973 that the MMR (measles, mumps, and rubella) vaccine and oral polio vaccine were contaminated with bacteriophages (viruses that eat bacteria). This was due to the blood used to make those vaccines containing bacteria, and the bacteria but not their attached bacteriophages being filtered out of the final product.
• In 1995, the MMR and yellow fever vaccines were found to be contaminated with the Endogenous Avian Retrovirus and the Avian Leukosis Virus.
• In 1997, scrapie was also spread to sheep through another contaminated vaccine.
• In 2004 and 2005, two rotavirus vaccines, Rotarix manufactured by GlaxoSmithKline (GSK) and RotaTeq manufactured by Merck, were found to be contaminated with porcine circovirus-1 (PCV1) after over 100 million doses of the vaccine had been distributed worldwide.
• In 2007, over 1 million doses of the Haemophilus influenzae type b (Hib) vaccine were recalled due to the detection of Bacillus cereus in the manufacturing equipment.
Sadly, as we investigate the past, it will become clear these events were only the tip of the iceberg.
Note: many reported incidents that I am not aware of didn't make it to this article, while a far larger number of incidents were never reported, but I nonetheless believe the cases listed in this article are more than sufficient to make the point. Similarly, as a I discussed in a previous article, while lab leaks with dangerous pathogens are typically not reported, enough documented instances exist within the peer reviewed literature to establish that those leaks are inevitable and impossible to avoid (which in turn argues that this research ever being conducted).
Sir Graham Wilson
Sir Graham Wilson was an eminent bacteriologist from the London School of Hygiene (e.g., in 1923 he coined the concept of herd immunity-an often impossible benchmark that I've previously shown has been used to repeatedly sell dubious vaccines to the world). Wilson grew up in a time when many bacterial infections were treated with vaccines or antiserums (particularly antitoxins for the tetanus or diphtheria toxin). At this time, his profession believed anti-vaxxers were irrational and pseudoscientific individuals and that vaccines were "100% safe and effective."
However, as Wilson became older, he began to see more and more evidence that there were real dangers to vaccination, and that his profession habitually covered it up to maintain the mythology all vaccines were "safe and effective." In turn, due to Wilson's stature in the field, many other (anonymous) vaccine experts shared their records of secret vaccine disasters that had occurred with Wilson and helped him to compile a detailed record of published and unpublished vaccine catastrophes that had occurred as many of them harbored immense guilt over what had happened, but simultaneously felt that they could not take on the risk of speaking publicly about it.
From reviewing the record he put together, what I find remarkable about Wilson's work was how much of it mirrors what we saw a century later-for example, very few people know that one of the original cases of Guillain Barré syndrome was due to a vaccine injury:
In an article published in 1919 Guillain and Barré referred to Landry's-type paralysis when they reported a fatal case of acute polyneuritis with albuminocytologic dissociation after typhoid vaccination.
In Guillain and Barré's case numbness and stiffness became apparent in the patient's legs the day after injection and the following day in his hands. Paralysis gradually came on and by the 9th day was complete in the legs, arms, and face. Bulbar symptoms developed on the 7th day, and on the 10th day, the patient died.
Note: previously I discussed many of the documented cases Wilson unearthed of a vaccination causing a pre-existing illness (e.g., polio) to spiral out of control.
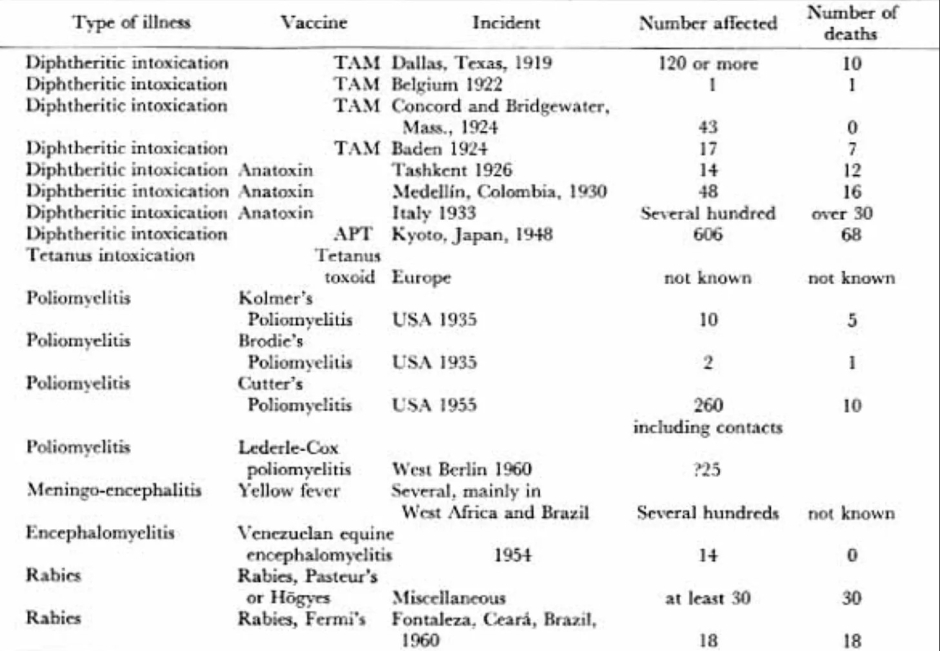
One of the key themes that kept on recurring in the records Wilson unearthed was that many vaccine catastrophes occurred after a contaminated lot was given to a large number of people (typically children or soldiers). Wilson in turn argued that rather than denying these incidents occurred, his profession needed to be honest about them so that the mistakes that led to these toxic 'hot' lots could be recognized and hence prevented from happening again. In The Hazards of Immunization, he discussed the following hot lot incidents:
I will now review those incidents in detail.
Note: Wilson documented many severe reactions that occurred from the early vaccinations. In this article, I am only covering the subset of reactions which occurred at a higher rate than the typical rate.
Hot Lots of the Past
Note: I tried to find all the sources Wilson cited (his citations were not that clear). For those not cited, please refer to his 1967 book. Additionally, some of the incidents listed here we not covered by Wilson, and for all of those, direct sources are provided. Lastly, many of the deaths described here were agonizing and horrific, but for brevity, I have not detailed each of them.
Diphtheria
Early diphtheria vaccines utilized the diphtheria toxin to provoke an immune response to it. Since it was so difficult to neutralize its toxicity, numerous accidents occurred due to hot lots being released with an active diphtheria toxin which had a variety of characteristic symptoms (many of which overlapped with other vaccine injuries). For example:
Disturbances of sensibility were sometimes detectable, especially in the older children. They included paraesthesia, formication in the extremities, and diminution in the muscular sense and the orientation of the limbs leading to ataxia. The patellar reflex was first exaggerated, then lost, and regained as recovery took place. One of the earliest symptoms was an exaggeration of the oculocardiac reflex; in several hundred patients it was observed that compression of the eyeball led to stoppage of the heart.
Note: the oculocardiac reflex is now a mostly a forgotten side of medicine (outside of very specific areas of medicine such as surgeries on the eyes). The diagnosis of this reflex is defined by the heart rate decreasing by over 20% after pressure is placed on the eyes (which typically does not happen) due to activation of the vagus nerve. I have a few theories on why vaccine injuries would cause that reflex to stop the heart, but I am not confident in any of them.
Let's now look at a few of the cases of diphtheria hot lots:
• In October 1919 the city of Dallas Texas began administering the diphtheria toxin (and its antitoxin) to non-immune children. Many different lots were used, and one of those ended up being hot (due to it having over 50 times the maximum permissible levels of free diphtheria toxin). Several hundred doses of it were given (although the exact number remains unknown), and 50 severe reactions to it were reported (with many more not being reported). When 120 of those injected were studied, it was found that 96 had reactions, 12 of which were moderate, 74 which were severe, and 10 of which were fatal.
Each of the 96 Dallas cases in turn had an almost identical progression of symptoms. Their symptoms went in the following order:
1. Intense burning at the site of injection which in a few hours became agonizing.
2. This was accompanied by severe nausea, vomiting, constipation, signs of a kidney injury, extreme swelling of the entire arm, and a reaction that spread into the rest of the body.
3. 24-48 hours after injections, vesicles appeared at the injection site, which leaked a burning fluid, and after they disappeared, left a raw ragged and ill-smelling patch 6-12 square inches (or more) in area which took around 2 to 2.5 months to heal.
4. Around 9-10 days, the heart became highly irregular and this lasted until the 8th to 10th week.
5. Starting at the third week, all the patients had muscles throughout the body become paralyzed (including the ones which controlled neurological functions like vision). Typically, these neurological complications lasted for 18-20 weeks, and tended to be more severe in those who had had a less severe initial reaction to the vaccine.
Remarkably, no investigation over what went wrong in Dallas was ever conducted, so other similar incidents also occurred.
Note: aspects of the incident are discussed within this 1927 book.
• In 1922 a 14-year old in Belgium was injected with a vial of diphtheria toxin (receiving at least 100 times the lethal dose) that had somehow gotten into a batch of tetanus vaccines, and died seven days later from cardiac paralysis.
• In Massachusetts in 1924, two lots were given that became toxic due to being frozen. For one lot, 21 of the 23 who received it, had severe reactions to the vaccine (but none died), while for the other lot, 22 of the 31 had severe reactions. After these incidents were studied, it was concluded that the cold had separated the antitoxin from caused it to agglomerate (clump) together on the bottom of the vial.
Note: colloidal agglomeration and zeta potential are discussed further here (as one of the primary toxicities of vaccines is that they cause fluids in the body like the blood to clump together and stop flowing).
• In Baden in 1924, 34 infants and children received a hot lot, of whom, 6 had no reaction, 11 had mild reactions, and 17 had severe reactions (of which 10 were fatal). A subsequent investigation revealed that when this lot was produced, diphtheria toxin was accidentally mixed with another diphtheria toxin rather than an antitoxin.
• In Tashkent (U.S.S.R.) in 1927, 14 children received diphtheria toxin instead of antitoxin, 8 of whom died. In their case, administering the antitoxin, appeared to prevent their immediate death and instead caused them to die from a progressive paralytic neurological disorder.
• In 1928 in Queensland, 21 children were injected with a diphtheria toxin-antitoxin mixture of whom 12 died. Unlike the other cases, this one appears to have been due to the vaccine being contaminated with Staph Aureus.
• In Columbia in 1930, 48 children were given toxin instead of antitoxin, many became severely ill (often becoming comatose or convulsive) and 16 of them (with 14 dying in 1-3 days and the others dying from progressive neurological symptoms). One noteworthy aspect of this incident was that many of the children developed the characteristic diphtheria membrane in the throat (which gradually suffocates you), suggesting that the toxin itself had an affinity for the throat (rather than just the infection) as no diphtheria bacteria could be found.
• In Italy, in 1933, several hundred infants and children became severely ill after being injected with a hot diphtheria lot, with over 30 dying.
Note: in most of these cases, autopsies also showed damage to organs throughout the body.
Once a safer way to produce the vaccine was discovered (using a toxoid rather than a toxin), production was shifted to the new method. However, incidents still happened with these newer vaccines. For example, in 1948 in Kyoto Japan, over 600 infants and children became ill from one lot, with at least 68 dying (along with 16 more deaths in Shimane). In one sample of 15,561 who received their second injection, 606 fell ill, and 68 died from muscular paralysis (with 59 dying in 1-2 weeks), and it was later discovered these hot lots again contained the free diphtheria toxin.
Given that children were regularly dying from diphtheria, I can understand why governments around the world believed any treatment for it was justified. Nonetheless, given that in each of these cases, the diphtheria toxin maintained a remarkably consistent lethal dose (roughly one-millionth of a gram) they should have done more to ensure that quality control was in place to prevent these agonizing deaths from happening. Sadly, as we've seen since then, that lesson still has not been learned.
Note: there was also a 1926 case in China where 33 of 89 people who received a diphtheria toxin antitoxin injection became ill (with 5 dying), from what appeared to be streptococci contamination. Subsequent investigation revealed that the source of this contamination was likely the distilled water used to dilute it.